- Home
- Media Kit
- Current Issue
- Past Issues
- Ad Specs-Submission
- Ad Print Settings
- Reprints (PDF)
- Photo Specifications (PDF)
- Contact Us

Loading
![]()
ONLINE


Kenneth L. Davis
Value in
Healthcare
Editors’ Note
Dr. Kenneth Davis attended the Icahn School of Medicine at Mount Sinai and completed a residency and fellowship in psychiatry and pharmacology, respectively, at Stanford University Medical Center. Upon returning to Mount Sinai, he became Chief of Psychiatry at the Mount Sinai-affiliated Bronx Veterans Administration Medical Center and launched Mount Sinai’s research program in the biology of schizophrenia and Alzheimer’s disease therapeutics. Davis was appointed CEO of The Mount Sinai Medical Center in 2003 after spending 15 years as Chair of Mount Sinai’s Department of Psychiatry. He was the first director for many of the institution’s research entities and received one of the first and largest program project grants for Alzheimer’s disease research from the National Institutes of Health. Davis also served as Dean of the Icahn School of Medicine at Mount Sinai from 2003 to 2007 and as President of the American College of Neuropsychopharmacology in 2006. In 2002, he was elected to the Institute of Medicine of the National Academy of Sciences, and in 2009, his undergraduate alma mater, Yale University, presented him with the George H. W. Bush ’48 Lifetime of Leadership Award.
Institution Brief
The Mount Sinai Health System (mountsinai.org) encompasses the Icahn School of Medicine at Mount Sinai and seven hospitals, as well as a large and expanding ambulatory care network. The seven hospitals – Mount Sinai Beth Israel, Mount Sinai Brooklyn, The Mount Sinai Hospital, Mount Sinai Queens, Mount Sinai St. Luke’s, Mount Sinai West, and the New York Eye and Ear Infirmary of Mount Sinai – have a vast geographic footprint throughout New York City. In 2015, Mount Sinai Health System hospitals received roughly four million patient visits, including inpatients, outpatients, and the emergency department.
The Icahn School of Medicine at Mount Sinai opened in 1968 and has more than 5,600 faculty members in 34 academic departments and 29 clinical and research institutes. A renowned medical school, it is ranked number two in the nation among medical schools for National Institutes of Health (NIH) funding per principal investigator. The Mount Sinai Hospital is ranked number 15 in the nation by U.S. News & World Report and ranked in the top 20 nationally in seven medical specialties in the 2016-17 “Best Hospitals” guidebook. The New York Eye and Ear Infirmary of Mount Sinai was also ranked nationally (number 10 in Ophthalmology). Mount Sinai Beth Israel, Mount Sinai St. Luke’s, and Mount Sinai West were ranked regionally.
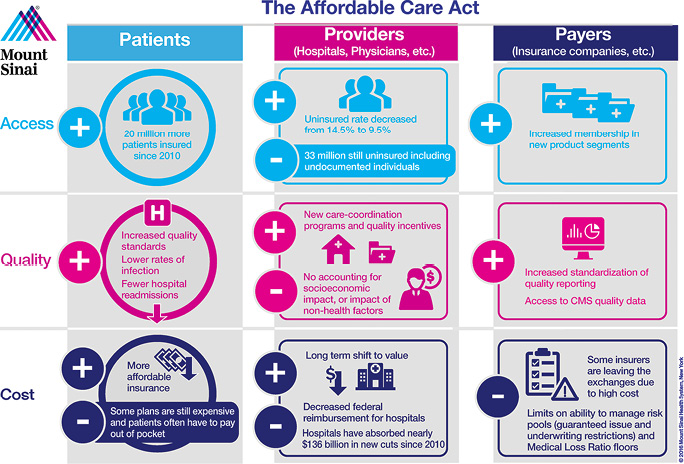
In terms of the impact the Affordable Care Act has had, has it been effective overall and what is the state of healthcare today?
The Affordable Care Act attempted to improve access, improve quality, and decrease the rate of cost. Those are three outcomes that it sought.
Those three outcomes affected three different groups: the patients, the providers, and the payers.
Looking at the patients, providers, and payers times quality, access, and cost, we have a three by three matrix with nine boxes. Depending on the box that one looks at, there is a different answer for each.
In terms of the most glaring example – access and patients – it’s a big positive. We have nearly 20 million more people who have insurance than had it before. We dropped the uninsured rate from about 14.5 to 9.5 percent of the population. President Obama just wrote a piece in JAMA that speaks to those advantages.
If we take a different box, for example providers and cost, in that box we conclude that providers, at least at Mount Sinai, because of things that happen not just in the ACA and with Obamacare but also things that have been done by CMS over the past five-plus years, we have significantly less revenue, and the providers of care seeing a whole lot less revenue is a huge challenge.
If we take the patients and quality box, clearly we have improved quality because there are all the penalties around quality. From the hospital’s point of view, it’s good that we have improved quality but no one was happy to do it at the expense of penalties rather than incentives.
Going forward, when it comes to what we have to learn and what we have to do to improve things, one of the things we’ve learned is the risk pools are not very favorable in the exchanges for a lot of the insurers; and the risk pools aren’t that favorable because the actuarial risk hasn’t been distributed in the way it might have been. That is because young healthy people have chosen to be penalized rather than to buy insurance.
That happened because the mandate’s penalties were very modest and don’t become more meaningful economically for some future years down the road.
We have risk pools that are certainly less than ideal that have caused the cost of the insurance to be higher than one would have hoped because we’re dealing with a sicker population of people.
Another factor that contributed to those problems is the ease with which there were exemptions for people to join after the deadlines for the exchanges.
Is it hard to be optimistic with all of the challenges facing healthcare?
It’s because of those challenges we have taken an aggressive stance towards moving away from fee-for-service contracts and moving increasingly towards value and risk, and population management.
We do that because we know in New York State there are particular inefficiencies in the system that are almost culturally ingrained that started in some decades-old training programs. For example, in some of the best academic medical centers, we would teach our house staff if they just think they need a test for any reason just to do it. We superimpose on that the difficulties in some of our less fortunate populations that have poor healthcare outcomes for a number of reasons. We see the need for care coordination and the opportunity that care coordination provides.
We think that at least in the near to intermediate term, if we can make the pivot to value, staff it appropriately, and get fair contracts, there is opportunity for us still to prosper in the marketplace. But this is a time of great anxiety.
With the consolidation taking place in the industry, will there be a handful of very large healthcare systems that survive?
To the degree that the FTC allows consolidation, the hospital industry will be inexorably driven toward that because margins are shrinking and the only way to recapture some margin is to provide more back-room, corporate efficiencies.
When smaller hospitals join systems and systems can provide services and centers of excellence, if those centers aren’t that far removed in distance from the initial community hospital, everybody wins, including the patients who, because they wind up in centers of excellence with higher volume, get better outcomes.•